
 USA
USA Brazil
Brazil China
China Croatia
Croatia Europe
Europe France
France Germany
Germany Italy
Italy Japan
Japan Latin America
Latin America Netherlands
Netherlands Spain
Spain Turkey
Turkey




By Leo Tjäderhane; DDS, PhD, professor of Cariology and Endodontics.
Have you ever had a Class V cavity preparation right at the gingival margin ready to be restored, when the gingiva starts bleeding heavily? Several hemostatic agents are supposed to stop bleeding, and they do – but if you even slightly touch the gingiva with your instrument the bleeding starts again. Frustrating, isn’t it? Unless you are extremely careful and very lucky, the restoration may easily be ruined (Fig. 1). At least, your day is ruined.
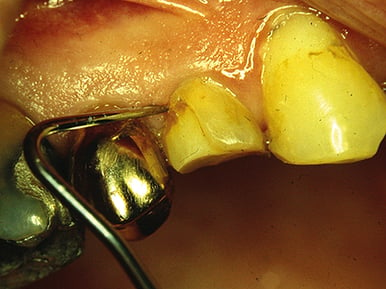
Fig. 1. Blood stain at the marginal third of a composite resin filling in a premolar, accompanied with a 1-mm gap at the gingival margin. The restoration is less than 6 months old. Photo by Leo Tjäderhane.
Actually, hemostatic agents – at least the best of them – work very well if we use them correctly. Let me share with you a clinical trick I learned from Dr. Dan Fischer more than 20 years ago, which I’ve been successfully practicing since.
Hemostatic agents are coagulants, causing the agglutination of blood proteins. The reaction is instant, but the mere contact of the agents with the bleeding surface results in only superficial coagulation. And this is where we dentists often make the first mistake. We are afraid of damaging the gingiva, thus we only gently apply the agent e.g. with a plastic brush tip or with the tip of the instrument. Alternatively, we may place a cord soaked in the agent into the bleeding sulcus. Both techniques are rather ineffective, since the effect of the small amount of agent is overwhelmed by the constant bleeding. Even if the bleeding seems to stop, the slight touch of an instrument, placing the matrix band, or applying the etchant gel easily provokes it again.
The trick to profound hemostasis is simple: scrubbing of copious amounts of hemostatic agent against the bleeding tissue. Scrubbing removes the superficial coagulum, ensures that fresh agent is constantly available to meet the blood oozing from the capillaries, and forces the coagulum deeper into the capillary openings – as long as there is enough agent to meet the challenge. Combining the ease of application with scrubbing force is most effectively achieved with a Metal Dento-InfusorTM tip (Ultradent Products, Inc.) (Fig. 2) connected into a Luer-Lock syringe containing AstringedentTM 15.5% ferric sulfate (Ultradent Products, Inc.) or AstringedentTM X 12.7% iron solution (Ultradent Products, Inc.), allowing constant and controlled application of the hemostatic agent during scrubbing (in close contact with the bleeding capillaries) (Fig. 3). The scrubbing force required is approximately equal to that required to scratch a lottery ticket.

Fig. 2. Metal Dento-InfusorTM tip allows delivery of pressure and a brush for scrubbing. Photo by Ultradent Products, Inc.
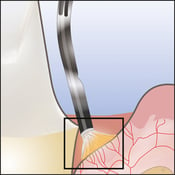


Fig. 3. Metal Dento-InfusorTM tip delivering the hemostatic agent right at the orifices of the bleeding capillaries. Constant application of the hemostatic agent with the pressure and brushing movement, creates the coagulum that closes the capillary orifices. Photos by Ultradent Products, Inc.
After 5-10 secs. of scrubbing, depending on the extent of bleeding, the gingival margin is washed, not only to remove the coagulum but also to test the hemostatic effect. This is the step in which we dentist often make the second mistake. Being afraid to introduce new bleeding, we tend to be too cautious with our washing. Instead, we need to wash vigorously to remove all loose coagulum and to reveal the areas where bleeding may still occur (Fig. 4). Only then are we able to identify the areas where the capillaries are incompletely blocked, where further application of the agent and scrubbing is required. In most cases, no more than two rounds are needed to achieve profound hemostasis for the whole working area. Then we are ready to continue with the restorative procedure.

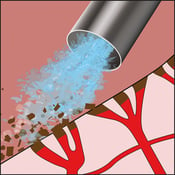

Fig. 4. Vigorous washing effectively removes the loose coagulum that could mask slight bleeding underneath. The gingival margin is dried with the air/-water syringe and observed in case some localized bleeding still occurs, which and requires further scrubbing of the hemostatic agent. Photos by Ultradent Products, Inc. (middle) and Dr. Jessop (right and left).
At this point, retraction cord can be placed if needed (Fig. 5). It can be soaked with the hemostatic agent; though my personal preference is to use it dry whenever possible. Placing the cord into a bleeding sulcus is both difficult and, in many cases, ineffective since the hemostatic effect of a relatively small amount of agent soon wears out.

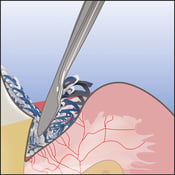

Fig. 5. Retraction cord, dry or soaked with the hemostatic agent, is easy to place when the sulcus is no longer bleeding. In many cases, the cord helps placing the marginal side of the cervical matrix correctly after applying the restorative material. Photos by Ultradent Products, Inc. (middle) and Dr. Jessop (right and left).
The ”scrub and wash” technique helps to achieve complete and long-lasting hemostasis in less than a minute, even in the most vigorously bleeding and inflamed gingival tissue. The tissue will now tolerate a matrix, etching acid and adhesives without the risk of bleeding. Time well spent to ensure conditions that allow high-quality restorative work.
Hemostatic agents and coagulum remnants have been suggested to affect the bonding strength1,2 and marginal integrity 2 of the restoration. With ferric sulfate, acid etching is sufficient to remove the potential remnants to allow appropriate bonding 2 and good marginal adaptation 3. When self-etch adhesives are used, cleaning the surface with ConsepsisTM Scrub (Ultradent Products, Inc.) containing 2% chlorhexidine gluconate is a safe way to combine the cleaning of the surface with the potential prevention of the hybrid layer collagen against collagenolytic enzymes 4.
You may wonder if you should worry about damaging the gingival tissue with rather vigorous scrubbing. Well, don’t worry! You cannot damage the gingival epithelium. It has a tensile strength of approximately 4 MPa5. If mechanical force could cause permanent damage to gingiva, we couldn’t treat periodontitis. If something comes loose during your scrubbing, it is inflammatory granulation tissue and the patient is better off without it.